Your Case Mix Index (CMI) is arguably the most critical health marker of your hospital’s financial profile. Yet, for many community and regional healthcare systems, this number is quietly stagnating.
The issue isn't that your patients aren't sick enough or that your doctors are bad at their jobs. The problem is a fundamental "translation gap" between the clinical reality at the bedside and the coded claims submitted to payers. When the complexity of care isn't captured in the data, your hospital loses out on essential reimbursement.
For a hospital discharging 10,000 Medicare patients per year, a CMI difference of just 0.10 can represent $2 to $4 million in annual revenue. This is not a rounding error; it is real money sitting in the gap between what your physicians documented and what your coders captured.
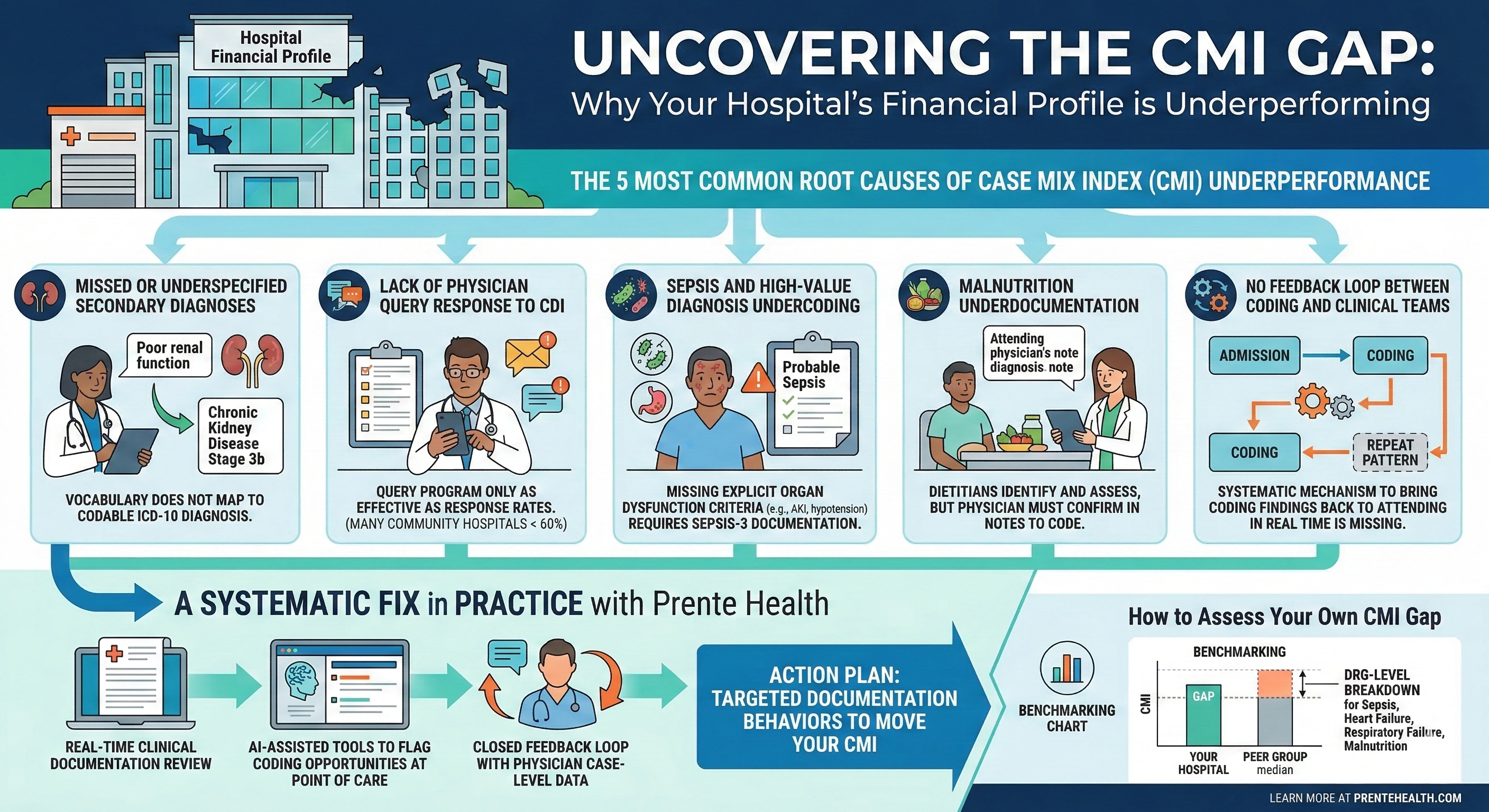
1. The Specificity Gap in Secondary Diagnoses
DRG assignment doesn't just rely on the primary reason for admission. It is heavily influenced by Complications and Comorbidities (CCs) and Major Complications and Comorbidities (MCCs).
A patient admitted for heart failure who also has Stage 3b chronic kidney disease and protein-calorie malnutrition represents a much higher resource intensity than a patient with heart failure alone. However, if the documentation only lists "poor renal function" or "low appetite," those secondary conditions won't map to a weighted code.
The Fix: Transition physician documentation from clinical descriptors to ICD-10-compliant diagnoses. Precision in vocabulary is the difference between a standard discharge and an appropriately weighted one.
2. The Friction in CDI Query Workflows
Clinical Documentation Improvement (CDI) programs are designed to bridge the gap between medicine and coding, but a program is only as strong as its response rate. In many facilities, physician query response rates hover below 60%.
When 40% of clarification requests go unanswered, millions in legitimate revenue are left on the table. This usually happens because physicians are busy, queries feel like administrative noise, and there is no immediate feedback loop showing how documentation affects reimbursement.
3. Sepsis-3 and the High-Value Coding Trap
Sepsis remains one of the largest opportunities for CMI accuracy, but it is also a compliance minefield. With the shift to Sepsis-3 criteria, payers now demand explicit evidence of organ dysfunction, such as acute kidney injury, altered mental status, or hypotension requiring vasopressors.
If a physician documents "probable sepsis" without linking it to specific organ failure, the case often defaults to a lower-weighted infection code. Over hundreds of annual admissions, this single documentation habit can drastically suppress your CMI.
4. The "Missing" Malnutrition MCC
Malnutrition is one of the most frequently overlooked MCCs in U.S. hospitals. While dietitians often identify malnutrition using ASPEN/AND criteria, their notes cannot be used for coding purposes unless the attending physician explicitly confirms the diagnosis in the medical record.
This is a classic workflow failure. If your clinical assessment and medical documentation aren't aligned, you are essentially providing high-intensity care without the corresponding reimbursement.
5. The Lack of a Feedback Loop
Traditional coding is often a black box where the chart is finished, the code is assigned, and the claim is sent. Physicians rarely hear back about how their documentation impacted the final DRG.
Without a real-time feedback loop, documentation errors simply repeat. A systematic fix involves bringing coding insights back to the point of care. Physicians who see the direct financial impact of their documentation choices are far more likely to improve their habits.
How to Measure Your CMI Gap
To see if your facility is underperforming, start by benchmarking your CMI against peers of similar size and payer mix using CMS Hospital Compare data. If your CMI is 0.05 to 0.10 below the peer median, you likely have a documentation gap worth quantifying.
The next step is a DRG-level breakdown to see which MS-DRG families are pulling your CMI down. Sepsis, heart failure, and respiratory failure are typically the highest-yield areas for improvement.
A Systematic Solution with Prente Health
The most successful hospitals don’t just work harder; they use better data. Prente Health applies AI-driven DRG analysis to your discharge data to pinpoint exactly where CMI is leaking, whether it is by diagnosis category, service line, or attending physician.
The output is not just a report; it is an action plan. By identifying the specific documentation behaviors that need to change, we help you capture the true complexity of the care you provide.